
eMedicine Specialties > Pediatrics: General Medicine > Infectious Disease
Mononucleosis and Epstein-Barr Virus Infection
Updated: Oct 20, 2009
Introduction
Background
- Epstein-Barr virus (EBV), or human herpesvirus 4, is a gammaherpesvirus that infects more than 95% of the world's population. The most common manifestation of primary infection with this organism is acute infectious mononucleosis, a self-limited clinical syndrome that most frequently affects adolescents and young adults. Classic symptoms include sore throat, fever, and lymphadenopathy. Infection with Epstein-Barr virus in younger children is usually asymptomatic or mild. However, Epstein-Barr virus is also a human tumor virus, the first virus associated with human malignancy. Infection with Epstein-Barr virus is associated with lymphoproliferative disorders, especially in immunocompromised hosts, and is associated with various tumors, including nasopharyngeal carcinoma and Burkitt lymphoma.
- Acute infectious mononucleosis was first described in the late 19th century as acute glandular fever, an illness consisting of lymphadenopathy, fever, hepatosplenomegaly, malaise, and abdominal discomfort in adolescents and young adults. In 1920, Sprunt and associates applied the name infectious mononucleosis to cases of spontaneously resolving acute leukemia associated with blastlike cells in the blood. Downey described the lymphocyte morphology in 1923. In 1932, Paul and Bunnell discovered that serum from symptomatic patients had antibodies that agglutinate the RBCs of unrelated species, the heterophile antibodies. This allowed enhanced diagnostic accuracy of infectious mononucleosis.
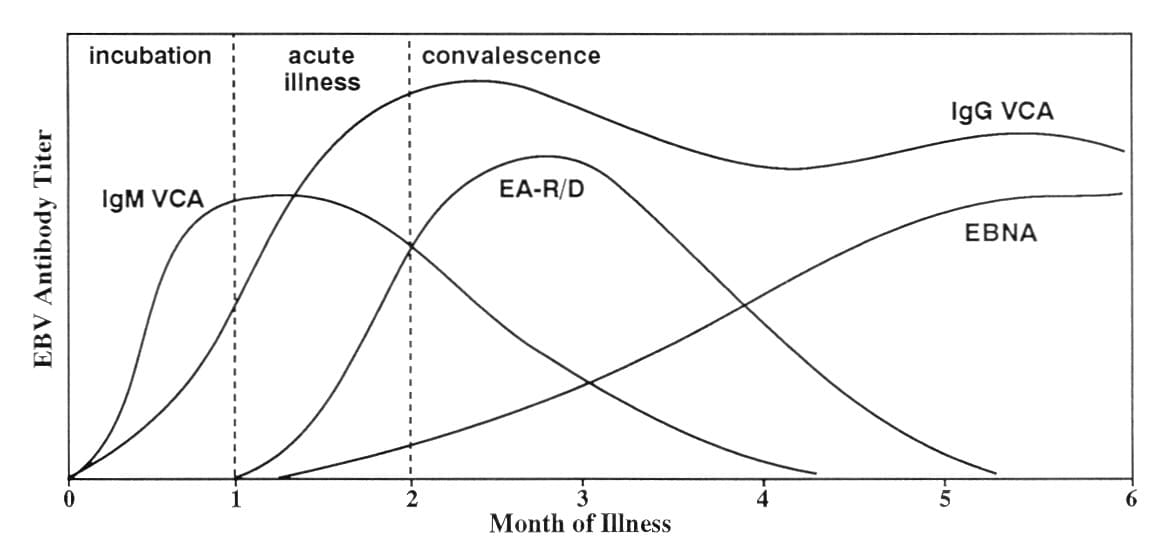
Infectious mononucleosis. Antibody response to Epstein-Barr virus. Adapted with permission from Johnson DH, Cunha BA. Epstein-Barr virus serology. Infect Dis Pract. 1995;19:26-27.
- The search for the etiologic agent of infectious mononucleosis was unsuccessful for many years, partly because researchers did not appreciate that most primary infections are asymptomatic and that most adults are seropositive. In 1964, Epstein described the first human tumor virus when he found virus particles in a Burkitt lymphoma cell line.1 Henle reported the relationship between acute infectious mononucleosis and Epstein-Barr virus in 1968.2 Subsequently, a large prospective study of students at Yale University firmly established Epstein-Barr virus as the etiologic agent of infectious mononucleosis.3
Pathophysiology
- Humans are the only known reservoir of Epstein-Barr virus. Epstein-Barr virus is present in oropharyngeal secretions and is most commonly transmitted through saliva. After initial inoculation, the virus replicates in nasopharyngeal epithelial cells. Cell lysis is associated with a release of virions, with viral spread to contiguous structures, including salivary glands and oropharyngeal lymphoid tissues. Further viral replication results in viremia, with subsequent infection of the lymphoreticular system, including the liver, spleen, and B lymphocytes in peripheral blood. Host immune response to the viral infection includes CD8+ T lymphocytes with suppressor and cytotoxic functions, the characteristic atypical lymphocytes found in the peripheral blood. The T lymphocytes are cytotoxic to the Epstein-Barr virus–infected B cells and eventually reduce the number of Epstein-Barr virus–infected B lymphocytes to less than 1 per 10^6 circulating B cells.
- Primary infection with Epstein-Barr virus is followed by latent infection, a characteristic of herpesviruses. After acute Epstein-Barr virus infection, latently infected lymphocytes and epithelial cells persist and are immortalized. In vivo, this allows perpetuation of infection, while, in vitro, immortalized cell lines are established. During latent infection, the virus is present in the lymphocytes and oropharyngeal epithelial cells as episomes in the nucleus. These episomes rarely integrate into the cell genome but do replicate with cell division and are passed to subsequent generations of cells. The rate of viral reactivation within the population of latently infected cells is low. Epithelial cells are the primary source of new virus in latently infected individuals, infecting B cells as they circulate through the oropharynx.
- Two strains, labeled EBV-1 and EBV-2 (also known as type A and type B), are observed. Although the genes expressed during latent infection have some differences, the acute illnesses caused by the 2 strains are apparently identical. Both strains are prevalent throughout the world and can simultaneously infect the same person.
- Knowledge of the structure of Epstein-Barr virus and of which proteins are expressed during different stages of its life cycle is required to understand the laboratory tests used to determine if an individual has primary acute, convalescent, latent, or reactivation infection. A mature infectious viral particle, which may be present in the cytoplasm of an epithelial cell, consists of a nucleoid, a capsid, and an envelope. The nucleoid contains linear double-stranded viral DNA. It is surrounded by the capsid, an icosahedral constructed of capsomers, which are tubular protein subunits. An envelope derived either from the outer membrane or the nuclear membrane of the host cell encloses the capsid and nucleoid (ie, the nucleocapsid). The envelope also contains viral proteins that were constructed and placed in the host cell membrane before viral assembly began.
- To initiate cellular infection, a viral particle attaches via its major outer envelope glycoprotein (ie, gp350/220) to the Epstein-Barr virus receptor CD21 on a B lymphocyte. The binding site on epithelial cells also may be CD21, but this has not been confirmed. Epstein-Barr virus is then internalized into cytoplasmic vesicles. After fusion of virus envelope with the vesicle membrane, the nucleocapsid is released into the cytoplasm. The nucleocapsid dissolves, the genome is transported to the cell nucleus, and the linear genome then circularizes, forming an episome. The cell may then proceed with either lytic infection with release of infectious virus or latent infection of the host cell. B lymphocytes with latent infection undergo growth transformation.
- Lytic infection occurs early after primary inoculation. As a result of lytic infection in oral epithelial cells, Epstein-Barr virus can be found in the saliva for the first 12-18 months after acquisition. Thereafter, epithelial cells and lymphocytes are latently infected, with a few spontaneously converting, leading to viral replication, host cell lysis and death, and release of mature virions. Thus, the virus can be isolated from oral secretions of 20-30% of healthy latently infected individuals at any time.
- During latent infection, cell proteins are expressed in 1 of 3 patterns. Type I latency, associated with Burkitt lymphoma, is characterized by expression of only Epstein-Barr virus–encoded RNAs, Epstein-Barr early regions (EBERs), and Epstein-Barr nuclear antigen 1 (EBNA1). Type II latency, associated with nasopharyngeal carcinoma, is characterized by expression of 3 latent membrane proteins (LMP1, LMP2A, LMP2B), plus EBERs and EBNA1. Type III latency is the pattern found in healthy individuals with latent infection. In addition to the EBERs and EBNA1 expressed in type I latency, other nuclear antigens (including EBNA2, EBNA3A, EBNA3B, EBNA3C, and LMP) are expressed in type III latency.
Frequency
United States
- Epstein-Barr virus is not a reportable infection, and the exact frequency of symptomatic primary infection is not known. By age 5 years, approximately 50% of the US population is infected. During childhood, primary infection is usually asymptomatic or associated with mild elevation of liver function test findings. Epstein-Barr virus infection acquired during adolescence is asymptomatic or associated with the syndrome of acute infectious mononucleosis.
- The incidence of acute infectious mononucleosis was approximately 45 cases per 100,000 population per year in the early 1970s, with the highest incidence in individuals aged 15-24 years. However, changes in economic status may have changed both the age of initial infection and the incidence of infectious mononucleosis since the large epidemiologic studies were completed. In lower socioeconomic groups, Epstein-Barr virus infection is more common, occurs at an earlier age, and is less likely to be associated with acute infectious mononucleosis.
- Roommates of students with primary Epstein-Barr virus infection develop seroconversion at the same rate as the general population of college students.
- Approximately 90% of the US population is infected with Epstein-Barr virus by age 25 years.
- Epstein-Barr virus infection does not occur in epidemics and has relatively low transmissibility.
International
- Epstein-Barr virus infection occurs with the same frequency and symptomatology in the developed nations of the world as in the United States.
- Epstein-Barr virus is more frequently acquired in childhood in underdeveloped nations, and, therefore, the syndrome of acute infectious mononucleosis is unusual in these nations.
- In Africa, the virus is associated with endemic Burkitt lymphoma in the setting of co-infection with Plasmodium falciparum.2
- High numbers of Epstein-Barr virus episomes are found in the cells of undifferentiated or poorly differentiated nasopharyngeal carcinoma. This is the most common tumor in adult men in southern China and is also common in North American Inuits and North African whites.
Mortality/Morbidity
- Most primary Epstein-Barr virus infections are asymptomatic. Death is unusual in immunocompetent patients with acute infectious mononucleosis but may occur due to neurologic complications, upper airway obstruction, or splenic rupture.
- Epstein-Barr virus infection is linked with numerous tumors.
- Endemic Burkitt lymphoma, the most common tumor of childhood in Africa, is associated with Epstein-Barr virus and malaria. Infection with P falciparum malaria stimulates polyclonal B-cell proliferation with Epstein-Barr virus infection and impairs the T-lymphocyte response to Epstein-Barr virus, apparently contributing to tumor pathogenesis.
- In Asia, Epstein-Barr virus infection is related to development of nasopharyngeal carcinoma. Predisposing factors include a diet rich in nitrosamines, salted fish, Chinese race, and the HLA-A2 haplotype.
- Most non-Hodgkin lymphomas are associated with Epstein-Barr virus, and evidence of the Epstein-Barr virus genome is demonstrable in many of these tumors.
- Epstein-Barr virus is also associated with Hodgkin lymphoma, in which the Epstein-Barr virus genome is present in the Reed-Sternberg cell. The EBNA1 protein interferes with tumor growth factor–beta signaling by downregulating Smad2; this interference with tumor-suppressor functions may contribute to tumor formation.4 In addition, the same protein may play a role in immune evasion via recruitment of regulatory T-helper cells.5 The precise mechanism by which Epstein-Barr virus may contribute to tumor pathogenesis are uncertain; some authors suggest that interleukin-10 may be linked to immune evasion, whereas others suggest it is linked to recovery.
- Epstein-Barr virus infection in patients who are immunocompromised is associated with several syndromes and proliferative disorders.
- Individuals with Duncan syndrome (ie, X-linked lymphoproliferative syndrome) may develop fatal primary Epstein-Barr virus infection due to a defect in the immune response to Epstein-Barr virus (poor anti-EBNA responses).
- The defective gene is the signaling lymphocyte activation molecule (SLAM)–associated protein (SAP) and is found on the X chromosome.
- Boys with Duncan syndrome often develop fatal massive hepatitis, hemophagocytosis, or a disseminated lymphoproliferative disorder triggered by primary Epstein-Barr virus infection.
- The median age of presentation is 2.5 years, with a median survival of 33 days. Survivors of the initial infection develop B-cell lymphoma or hypogammaglobulinemia and usually die by age 10 years.
- In children with Duncan Syndrome, the paucity of normal class-switched mature B cells means the virus instead establishes itself in nonswitched memory B cells (as opposed to naive or transitional B cells).6
- Other congenital immunodeficiencies are associated with the development of Epstein-Barr virus–associated lymphoproliferative disorders. These include ataxia-telangiectasia, Chédiak-Higashi syndrome, Wiskott-Aldrich syndrome, and common variable immunodeficiency.
- Posttransplant lymphoproliferative disorder (PTLD) is a potentially fatal lymphoproliferative syndrome associated with Epstein-Barr virus and monoclonal or polyclonal expansion of B cells. It occurs in patients after organ transplantation, particularly after heart transplantation, and usually responds to decreased immune suppression.
- Epstein-Barr virus–associated lymphomas occur in patients with secondary immunodeficiencies (eg, after cancer chemotherapy). Unfortunately, these tumors do not respond to decreased immunosuppression.
- In patients with AIDS, Epstein-Barr virus is associated with hairy leukoplakia, leiomyosarcoma, CNS lymphoma, and lymphoid interstitial pneumonitis in children. However, only approximately one half of acquired immunodeficiency syndrome (AIDS)-associated Burkitt lymphomas contain Epstein-Barr virus genomes, which suggests a more complex interaction between chronic human immunodeficiency virus (HIV) infection and immune system defects. Acyclovir has been shown to have some potential benefit in treating patients with AIDS-associated Epstein-Barr virus disease.
- Individuals with Duncan syndrome (ie, X-linked lymphoproliferative syndrome) may develop fatal primary Epstein-Barr virus infection due to a defect in the immune response to Epstein-Barr virus (poor anti-EBNA responses).
Race
- Epstein-Barr virus infection has no racial predilection; however, HLA-A2 haplotypes, which are more common in people of Chinese origin, are associated with a predisposition for nasopharyngeal carcinoma. The risk associated with HLA-A2 haplotypes is higher than any environmental risk posed by diet. First-generation US immigrants of Chinese origin have a higher risk for nasopharyngeal carcinoma.7
- Large epidemiologic studies performed in the 1970s revealed that acute infectious mononucleosis was 30 times more likely to occur in whites than in African Americans. However, this correlated with lower social economic status and earlier asymptomatic infection in African Americans and, therefore, did not reflect a true racial difference.
Sex
- The incidence of infectious mononucleosis is the same in men and women, although the peak incidence occurs 2 years earlier in females.
- Postinfectious fatigue is more common in females.8,9
Age
- Epstein-Barr virus infection usually occurs during infancy or childhood and remains latent through life.
- In developed nations, infection may not occur until adolescence or adulthood, and approximately 50% of adolescents who acquire Epstein-Barr virus develop the infectious mononucleosis syndrome.
- Acute infectious mononucleosis has been reported in middle-aged and elderly adults; these individuals are usually heterophile antibody negative.
Clinical
History
- Acute infectious mononucleosis presents with a history of 1-2 weeks of fatigue and malaise; however, onset may be abrupt.
- The incubation period in adolescents is 30-50 days; however, it is shorter in young children.
- Symptoms include sore throat, headache, fever, myalgias, nausea, and abdominal pain.
- Sore throat is the most frequent presenting symptom. Gradually worsening over the first week, it may be the most severe sore throat the patient has experienced.
- Headache usually occurs during the first week and may be retro-orbital.
- Left upper quadrant pain may be due to splenic enlargement. Abdominal pain should prompt suspicion of splenic rupture.
- Symptoms usually persist for 2-3 weeks, but fatigue is often more prolonged.
- Infants and young children with primary infection are usually asymptomatic.
Physical
Infectious mononucleosis is characterized by pharyngitis, generalized lymphadenopathy, and hepatosplenomegaly. Most clinical symptoms are due to T-cell proliferation and organ infiltration. Children younger than 4 years frequently have splenomegaly or hepatomegaly, rash, and symptoms of an upper respiratory tract infection.
- Pharyngitis
- Pharyngitis is exudative in one third of patients and is the most consistent physical finding.
- Petechiae are present at the junction of the hard and soft palates in 25-60% of patients.
- Tonsillar enlargement can be massive and occasionally causes airway obstruction. The enlargement can be associated with dehydration due to difficulty in swallowing.
- Lymphadenopathy
- Lymphadenopathy is prominent and most commonly affects the posterior cervical lymph nodes. Anterior cervical and submandibular nodal involvement is common, and axillary and inguinal nodes are also affected.
- Enlarged epitrochlear nodes are highly suggestive of infectious mononucleosis.
- Nodal enlargement is usually symmetric.
- Nodes are mildly tender to palpation and are freely moveable.
- Hepatomegaly: Although hepatomegaly is common, jaundice is rare. Percussion tenderness over the liver is common.
- Splenomegaly
- Splenomegaly is common. The spleen is often palpable 2-3 cm below the left costal margin and may be tender.
- The spleen rapidly enlarges over the first week of symptoms, usually decreasing in size over the next 7-10 days.
- The spleen can rupture from relatively minor trauma or even spontaneously.
- Fever: More than 90% of patients develop fever, which is most severe in the afternoon, typically peaking at 38-39°C, but it may reach 40°C. Fever resolves over 10-14 days. Despite fever, the pulse is usually normal or relatively low, and tachycardia is unusual.
- Maculopapular rash: A usually faint, widely scattered, and erythematous maculopapular rash occurs in 3-15% of patients and is more common in young children.
- Treatment with amoxicillin or ampicillin is associated with rash in approximately 80% of patients. This is often encountered when primary Epstein-Barr virus (EBV) infection is initially misdiagnosed as strep throat and is treated as such.
- Circulating immunoglobulin G (IgG) and immunoglobulin M (IgM) antibodies to ampicillin are observed.
- Eyelid edema: This may be present, especially in the first week of illness.
- Genital ulcers have been described in girls and may be confused with genital herpes.10
Causes
- Epstein-Barr virus is the etiologic agent in approximately 90% of acute infectious mononucleosis cases.
- Cytomegalovirus (CMV), another herpesvirus, is most commonly associated with Epstein-Barr virus–negative infectious mononucleosis syndrome.
- Other viruses associated with a similar acute illness include adenovirus; hepatitis A, hepatitis B, or hepatitis C; herpes simplex 1 and herpes simplex 2; human herpesvirus 6; rubella; and primary HIV in adolescents or young adults.
- The etiology of most Epstein-Barr virus–negative infectious mononucleosis cases remains unknown.
More on Mononucleosis and Epstein-Barr Virus Infection |
 Overview: Mononucleosis and Epstein-Barr Virus Infection Overview: Mononucleosis and Epstein-Barr Virus Infection |
| Differential Diagnoses & Workup: Mononucleosis and Epstein-Barr Virus Infection |
| Treatment & Medication: Mononucleosis and Epstein-Barr Virus Infection |
| Follow-up: Mononucleosis and Epstein-Barr Virus Infection |
| Multimedia: Mononucleosis and Epstein-Barr Virus Infection |
| References |
| Next Page » |
References
Epstein MA. Virus particles in cultured lymphoblasts from Burkitt's lymphoma. Lancet. 1964;1:702.
Henle G, Henle W, Diehl V. Relation of Burkitt's tumor-associated herpes-ytpe virus to infectious mononucleosis. Proc Natl Acad Sci U S A. Jan 1968;59(1):94-101. [Medline].
Sawyer RN, Evans AS, Niederman JC, McCollum RW. Prospective studies of a group of Yale University freshmen. I. Occurrence of infectious mononucleosis. J Infect Dis. Mar 1971;123(3):263-70. [Medline].
Flavell JR, Baumforth KR, Wood VH, et al. Down-regulation of the TGF-beta target gene, PTPRK, by the Epstein-Barr virus encoded EBNA1 contributes to the growth and survival of Hodgkin lymphoma cells. Blood. Jan 1 2008;111(1):292-301. [Medline]. [Full Text].
Baumforth KR, Birgersdotter A, Reynolds GM, et al. Expression of the Epstein-Barr virus-encoded Epstein-Barr virus nuclear antigen 1 in Hodgkin's lymphoma cells mediates Up-regulation of CCL20 and the migration of regulatory T cells. Am J Pathol. Jul 2008;173(1):195-204. [Medline]. [Full Text].
Chaganti S, Ma CS, Bell AI, et al. Epstein-Barr virus persistence in the absence of conventional memory B cells: IgM+IgD+CD27+ B cells harbor the virus in X-linked lymphoproliferative disease patients. Blood. Aug 1 2008;112(3):672-9. [Medline].
Lung ML, Chang GC, Miller TR, Wara WM, Phillips TL. Genotypic analysis of Epstein-Barr virus isolates associated with nasopharyngeal carcinoma in Chinese immigrants to the United States. Int J Cancer. Dec 15 1994;59(6):743-6. [Medline].
Katz BZ, Shiraishi Y, Mears CJ, Binns HJ, Taylor R. Chronic fatigue syndrome after infectious mononucleosis in adolescents. Pediatrics. Jul 2009;124(1):189-93. [Medline].
Candy B, Chalder T, Cleare AJ, et al. Predictors of fatigue following the onset of infectious mononucleosis. Psychol Med. Jul 2003;33(5):847-55. [Medline].
Halvorsen JA, Brevig T, Aas T, Skar AG, Slevolden EM, Moi H. Genital ulcers as initial manifestation of Epstein-Barr virus infection: two new cases and a review of the literature. Acta Derm Venereol. 2006;86(5):439-42. [Medline].
Michelson P, Watkins B, Webber SA, Wadowsky R, Michaels MG. Screening for PTLD in lung and heart-lung transplant recipients by measuring EBV DNA load in bronchoalveolar lavage fluid using real time PCR. Pediatr Transplant. Jun 2008;12(4):464-8. [Medline].
Candy B, Chalder T, Cleare AJ, Wessely S, Hotopf M. A randomised controlled trial of a psycho-educational intervention to aid recovery in infectious mononucleosis. J Psychosom Res. Jul 2004;57(1):89-94. [Medline].
Lockey TD, Zhan X, Surman S, Sample CE, Hurwitz JL. Epstein-Barr virus vaccine development: a lytic and latent protein cocktail. Front Biosci. May 1 2008;13:5916-27. [Medline]. [Full Text].
Aldrete JS. Spontaneous rupture of the spleen in patients with infectious mononucleosis. Mayo Clin Proc. Sep 1992;67(9):910-2. [Medline].
Andersson J, Britton S, Ernberg I, et al. Effect of acyclovir on infectious mononucleosis: a double-blind, placebo-controlled study. J Infect Dis. Feb 1986;153(2):283-90. [Medline].
Boyle GJ, Michaels MG, Webber SA, et al. Posttransplantation lymphoproliferative disorders in pediatric thoracic organ recipients. J Pediatr. Aug 1997;131(2):309-13. [Medline].
Cheeseman SH, Henle W, Rubin RH, et al. Epstein-Barr virus infection in renal transplant recipients. Effects of antithymocyte globulin and interferon. Ann Intern Med. Jul 1980;93(1):39-42. [Medline].
Collins M, Fleisher G, Kreisberg J, Fager S. Role of steroids in the treatment of infectious mononucleosis in the ambulatory college student. J Am Coll Health. Dec 1984;33(3):101-5. [Medline].
Connelly KP, DeWitt LD. Neurologic complications of infectious mononucleosis. Pediatr Neurol. May 1994;10(3):181-4. [Medline].
Copperman SM. "Alice in Wonderland" syndrome as a presenting symptom of infectious mononucleosis in children: a description of three affected young people. Clin Pediatr (Phila). Feb 1977;16(2):143-6. [Medline].
Cyran EM, Rowe JM, Bloom RE. Intravenous gammaglobulin treatment for immune thrombocytopenia associated with infectious mononucleosis. Am J Hematol. Oct 1991;38(2):124-9. [Medline].
Deacon EM, Pallesen G, Niedobitek G, et al. Epstein-Barr virus and Hodgkin's disease: transcriptional analysis of virus latency in the malignant cells. J Exp Med. Feb 1 1993;177(2):339-49. [Medline].
Dupre L, Andolfi G, Tangye SG, et al. SAP controls the cytolytic activity of CD8+ T cells against EBV-infected cells. Blood. Jun 1 2005;105(11):4383-9. [Medline]. [Full Text].
Erzurum S, Kalavsky SM, Watanakunakorn C. Acute cerebellar ataxia and hearing loss as initial symptoms of infectious mononucleosis. Arch Neurol. Nov 1983;40(12):760-2. [Medline].
Evans AS, Niederman JC, Cenabre LC, West B, Richards VA. A prospective evaluation of heterophile and Epstein-Barr virus-specific IgM antibody tests in clinical and subclinical infectious mononucleosis: Specificity and sensitivity of the tests and persistence of antibody. J Infect Dis. Nov 1975;132(5):546-54. [Medline].
Foerster J. Infectious mononucleosis. In: Lee. Wintrobe's Clinical Hematology. 10th ed. 1999:1926-1955.
Gasser O, Bihl FK, Wolbers M, et al. HIV Patients Developing Primary CNS Lymphoma Lack EBV-Specific CD4(+) T Cell Function Irrespective of Absolute CD4(+) T Cell Counts. PLoS Med. Mar 27 2007;4(3): e96.:[Medline]. [Full Text].
Green M, Bueno J, Rowe D, et al. Predictive negative value of persistent low Epstein-Barr virus viral load after intestinal transplantation in children. Transplantation. Aug 27 2000;70(4):593-6. [Medline].
Greenspan JS, Greenspan D, Lennette ET, et al. Replication of Epstein-Barr virus within the epithelial cells of oral "hairy" leukoplakia, an AIDS-associated lesion. N Engl J Med. Dec 19 1985;313(25):1564-71. [Medline].
Haller A, von Segesser L, Baumann PC, et al. Severe respiratory insufficiency complicating Epstein-Barr virus infection: case report and review. Clin Infect Dis. Jul 1995;21(1):206-9. [Medline].
Hanto DW. Classification of Epstein-Barr virus-associated posttransplant lymphoproliferative diseases: implications for understanding their pathogenesis and developing rational treatment strategies. Annu Rev Med. 1995;46:381-94. [Medline].
Heath CW Jr, Brodsky AL, Potolsky AI. Infectious mononucleosis in a general population. Am J Epidemiol. Jan 1972;95(1):46-52. [Medline].
Hickey SM, Strasburger VC. What every pediatrician should know about infectious mononucleosis in adolescents. Pediatr Clin North Am. Dec 1997;44(6):1541-56. [Medline].
Hsieh WC, Chang Y, Hsu MC, et al. Emergence of anti-red blood cell antibodies triggers red cell phagocytosis by activated macrophages in a rabbit model of epstein-barr virus-associated hemophagocytic syndrome. Am Jour Path. May 2007;170(5):1629-39. [Medline].
Klein G. Viral latency and transformation: the strategy of Epstein-Barr virus. Cell. Jul 14 1989;58(1):5-8. [Medline].
Liebowitz D. Nasopharyngeal carcinoma: the Epstein-Barr virus association. Semin Oncol. Jun 1994;21(3):376-81. [Medline].
Linderholm M, Boman J, Juto P, Linde A. Comparative evaluation of nine kits for rapid diagnosis of infectious mononucleosis and Epstein-Barr virus-specific serology. J Clin Microbiol. Jan 1994;32(1):259-61. [Medline].
Maddern BR, Werkhaven J, Wessel HB, Yunis E. Infectious mononucleosis with airway obstruction and multiple cranial nerve paresis. Otolaryngol Head Neck Surg. Apr 1991;104(4):529-32. [Medline].
Manika K, Alexiou-Daniel S, Papakosta D, et al. Epstein-Barr virus DNA in bronchoalveolar lavage fluid from patients with idiopathic pulmonary fibrosis. Sarcoidosis Vasc Diffuse Lung Dis. Sep 2007;24(2):134-40. [Medline].
Miller CS, Avdiushko SA, Kryscio RJ, Danaher RJ, Jacob RJ. Effect of prophylactic valacyclovir on the presence of human herpesvirus DNA in saliva of healthy individuals after dental treatment. J Clin Microbiol. 2005;43(5):2173-2180.
Navarro WH, Kaplan LD. AIDS-related lymphoproliferativedisease. Blood. 2006;107(1):13-20.
Okano M, Gross TG. Epstein-Barr virus-associated hemophagocytic syndrome and fatal infectious mononucleosis. Am J Hematol. Oct 1996;53(2):111-5. [Medline].
Pereira MS, Blake JM, Macrae AD. EB virus antibody at different ages. Br Med J. Nov 29 1969;4(5682):526-7. [Medline].
Petersen I, Thomas JM, Hamilton WT, White PD. Risk and predictors of fatigue after infectious mononucleosis in a large primary-care cohort. QJM. Jan 2006;99(1):49-55. [Medline].
Porter DD, Wimberly I, Benyesh-Melnick M. Prevalence of antibodies to EB virus and other herpesviruses. JAMA. Jun 2 1969;208(9):1675-9. [Medline].
Resnick L, Herbst JS, Ablashi DV, et al. Regression of oral hairy leukoplakia after orally administered acyclovir therapy. JAMA. Jan 15 1988;259(3):384-8. [Medline].
Rowe M, Lear AL, Croom-Carter D, Davies AH, Rickinson AB. Three pathways of Epstein-Barr virus gene activation from EBNA1-positive latency in B lymphocytes. J Virol. Jan 1992;66(1):122-31. [Medline].
Rowe M, Young LS, Cadwallader K, Petti L, Kieff E, Rickinson AB. Distinction between Epstein-Barr virus type A (EBNA 2A) and type B (EBNA 2B) isolates extends to the EBNA 3 family of nuclear proteins. J Virol. Mar 1989;63(3):1031-9. [Medline].
Schooley RT. Epstein-Barr virus (infectious mononucleosis). In: Mandell. Principles and Practice of Infectious Diseases. 5th ed. 2000:1599-1608.
Schooley RT, Carey RW, Miller G, et al. Chronic Epstein-Barr virus infection associated with fever and interstitial pneumonitis. Clinical and serologic features and response to antiviral chemotherapy. Ann Intern Med. May 1986;104(5):636-43. [Medline].
Straus SE, Cohen JI, Tosato G, Meier J. NIH conference. Epstein-Barr virus infections: biology, pathogenesis, and management. Ann Intern Med. Jan 1 1993;118(1):45-58. [Medline].
Thorley-Lawson DA. Basic virological aspects of Epstein-Barr virus infection. Semin Hematol. Jul 1988;25(3):247-60. [Medline].
Tomkinson BE, Wagner DK, Nelson DL, Sullivan JL. Activated lymphocytes during acute Epstein-Barr virus infection. J Immunol. Dec 1 1987;139(11):3802-7. [Medline].
Tosato G, Taga K, Angiolillo AL, Sgadari C. Epstein-Barr virus as an agent of haematological disease. Baillieres Clin Haematol. Mar 1995;8(1):165-99. [Medline].
Tynell E, Aurelius E, Brandell A, et al. Acyclovir and prednisolone treatment of acute infectious mononucleosis: a multicenter, double-blind, placebo-controlled study. J Infect Dis. Aug 1996;174(2):324-31. [Medline].
Vassallo M, Camilleri M, Caron BL, Low PA. Gastrointestinal motor dysfunction in acquired selective cholinergic dysautonomia associated with infectious mononucleosis. Gastroenterology. Jan 1991;100(1):252-8. [Medline].
Williams ML, Loughran TP Jr, Kidd PG, Starkebaum GA. Polyclonal proliferation of activated suppressor/cytotoxic T cells with transient depression of natural killer cell function in acute infectious mononucleosis. Clin Exp Immunol. Jul 1989;77(1):71-6. [Medline].
Further Reading
Keywords
mononucleosis, Epstein-Barr virus infection, EBV, acute infectious mononucleosis, infectious mononucleosis, mono, human herpesvirus 4, HHV-4, kissing disease, gamma-herpesvirus, human tumor virus, lymphoproliferative disorders, nasopharyngeal carcinoma, Burkitt lymphoma, endemic Burkitt lymphoma, acute glandular fever, non-Hodgkin lymphomas, Hodgkin lymphoma, Duncan syndrome, X-linked lymphoproliferative syndrome, fatal massive hepatitis, disseminated lymphoproliferative disorder, B-cell lymphoma, hypogammaglobulinemia, EBV-associated lymphoproliferative disorders, EBV-associated lymphomas, ataxia-telangiectasia, Chédiak-Higashi syndrome, Wiskott-Aldrich syndrome, posttransplant lymphoproliferative disorder, PTLD, lymphoproliferative syndrome, hairy leukoplakia, leiomyosarcoma, CNS lymphoma, lymphoid interstitial pneumonitis, infectious mononucleosis syndrome, sore throat, splenic rupture, pharyngitis, hepatosplenomegaly, petechiae, tonsillar enlargement, enlarged epitrochlear nodes, hepatomegaly, splenomegaly, maculopapular rash
 Saving Highlight
Saving Highlight
 Saving Hilight for you...
Saving Hilight for you...
 Un-highlight
Un-highlight








